Case Report Download PDF
An Unusual Presentation of Left Atrial Myxoma as One and A Half Syndrome
Received: June 20, 2019; Published: July 05, 2019
Abstract
Atrial myxomas are a rare cause of stroke, accounting for less than 1% of all ischemic strokes. Although rare, atrial myxoma should be considered in the differential diagnosis of any adult who presents with ischemic stroke. The embolic manifestation may be the initial presentation in many cases and if the tumour is not detected, may lead to recurrent ischemic events. Surgical removal of the myxoma is usually a permanent measure to prevent subsequent strokes. Here we present a rare presentation of ischemic stroke in the form of fisher’s one and half syndrome
Keywords: Myxoma; Stroke; One and Half Syndrome
Introduction
A fifty-nine-year-old euglycemic hypertensive came with complaints of stuttering of speech with weakness of right upper limb and lower limb with giddiness and visual disturbance for two days. No history of chest pain, breathlessness, fever, trauma. Clinical examination revealed right hemiparesis grade 3/5 with left Internuclear Ophthalmoplegia, Left Horizontal Gaze Palsy and normal convergence and right upper motor neuron type of facial palsy. Investigations were unremarkable except for MRI brain showing acute infarcts in left thalamus, sub-acute infarcts in both cerebellar hemispheres and vermis and chronic infarct in right caudate nucleus (Figure 1). Carotid Doppler was normal with no flow limiting lesion. Further search towards the focus of stroke came in the form of echo cardiography showing a mass of size 4*3 cm (Figure 2) attached to the lower part of inter atrial septum and atrial side of mitral valve protruding to LV through mitral valve during diastole. There was no Mitral Regurgitation and the ventricular function was good. Cardiac MRI also confirmed the similar findings (Figure 3). He was in sinus rhythm.
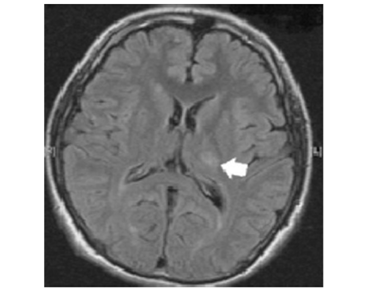
Figure 1: MRI of the brain showing acute infarct in the left thalamus as indicated by white arrow.
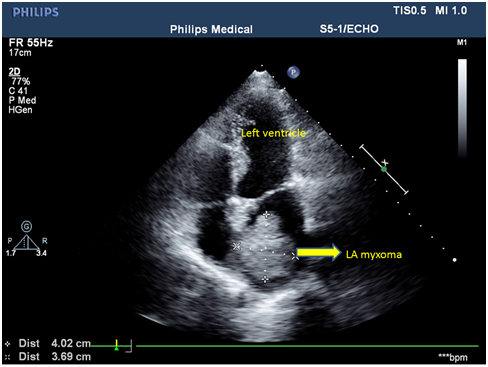
Figure 2: Apical four chamber view in echo showing left atrial myxoma.
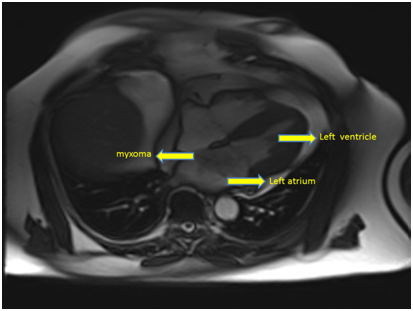
Figure 3: cardiac MRI showing left atrial myxoma.
Patient was planned for LA myxoma removal after six weeks for the recovery of stroke after obtaining neurology consultation. Clinically his neurological deficit improved with power in right side improving to 4+/5 with physiotherapy although the ocular findings remained the same. He was taken up for surgery and after doing median sternotomy and aortic bicaval cannulation, (there was no atheromatous plaque in the aorta on palpation and Transesophageal Echo also confirmed the same) LA was opened and the tumour was delineated and excised along the inter atrial septum. A 3*4 cm mass was found attached to the lower end of inter atrial septum and atrial side of mitral valve and was sent for biopsy which revealed myxoma. The resulting Atrial Septal Defect was closed with a pericardial patch. Surgery and the post-operative course was uneventful and the patient was discharged in stable condition after neurological improvement. The last follow up was at two years in which the patient was doing well with echo showing norecurrence of myxoma with neurologically complete recovery of the hemiparesis and better improvement in vision, and no residual facial palsy with persistent left horizontal gaze palsy
Discussion
In 1952, Goldberg et al reported the first ante mortem diagnosis of atrial myxoma in a 3-year-old who presented with a recurrent right hemiparesis [1]. In the last 35 years, several series of atrial myxomas have been reported. Classic presenting manifestations include constitutional, obstructive, and embolic symptoms. Constitutional symptoms, are reported in 30-89% of cases. Next comes the obstructive symptoms which are reported in 45% of cases [2]Neurologic manifestations of atrial myxomas are frequent and have been reported in 25-45% of cases. The neurologic signs and symptoms are usually a result of embolization. Emboli are most often myxomatous but may also arise from thrombus adherent to the tumor. Embolization from a left atrial myxoma has been reported to cause cerebral infarction in 27% of cases [3]. Myxomas are associated with ischemic and haemorrhagic cerebrovascular events, which are sequelae of tumor embolism into the brain. Ischemic stroke is the most frequent embolic manifestation of atrial myxoma. Within the brain, the middle cerebral artery and its branches are the most common sites of embolic occlusion [4]. Detection of the myxoma, followed by its resection, is the only currently recognized modality for preventing further ischemic strokes [4]. Multi-infarct dementia has been reported as a resultof recurrent cerebral embolization. Spinal cord embolus, resulting in paraplegia, has also been reported [5].
The “One-and-a-Half” syndrome was first described by Fisher in 1967. The disorder is characterized by a lateral gaze palsy in one direction with an Internuclear Ophthalmoplegia (INO) in the other direction [5]. In the complete form of the syndrome, the ipsilateral eye lies fixed at the midline for all lateral movements;the other eye can only abduct and exhibits horizontal jerk nystagmus in abduction. The syndrome is usually due to a unilateral lesion in the lower part of the dorsal pontine tegmentum affecting the ipsilateral Para median pontine reticular formation (PPRF), the abducens nucleus, and Internuclear fibres of the ipsilateral medial longitudinal fasciculus (MLF) [5]. In summary, cerebral emboli remain frequent presentations and complications of atrial myxomas. Atrial myxomas are relatively rare but should be considered in the differential diagnosis of cerebral infarction, particularly when multiple cerebral infarctions have occurred and constitutional symptoms are reported [5]. Cerebral infarction may occur before the onset of constitutional or obstructive symptoms [5]. Once detected, removal of an atrial myxoma should be considered urgent due to the great embolic potential of this condition. Improved imaging techniques such as gated cardiac MRI continue to facilitate the diagnosis of this potentially curable cause of stroke.
Conclusion
Atrial myxoma as a cause of One and a half syndrome is very rare and to our limited knowledge this is the first of its type presenting in this rare clinical entity. Hencewe emphasise that myxomas should be always kept in mind in such rare causes of stroke with an unusual presentation of neurological syndrome
References
- 1.Reynen K (1995) Cardiac myxomas.N Engl J Med 333:1610-1617.
- Pinede L, Duhaut P, Loire R (2001) Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore) 80:159-172.
- Ng HK, Poon WS (1990) Cardiac myxoma metastasizing to the brain: case report. J Neurosurg 72:295-298.
- Chen HJ, Liou CW, Chen L (1993) Metastatic atrial myxoma presenting as intracranial aneurysms with hemorrhage: case report. SurgNeurol 40:61-64.
- Knepper LE, Biller J, Adams HP Jr, Bruno A (1998) Neurologic manifestations of atrial myxoma. A 12-year experience and review. Stroke 19(11):1435-1440.